

Mark Lorenz
11 June, 2021
400
20
UsingBlueButton2.0-IfIRanaHealthPlan
In this post:
- Live proof-of-concept connection to Blue Button 2.0 for you to test.
- An overview of how Medicare Advantage plans are paid.
- What if I ran a zoo?
A favorite bed time story book in our house is "If I Ran a Zoo" by Dr. Seuss. If you don't have children, and also didn't have a childhood- this is a story about a naive boy who visits a perfectly good zoo, and decides he could do way better by adding a bunch of ridiculous animals that don't even exist- which is a perfect parallel for this blog post.
What are "patient access APIs"? Read my post about the basics to catch up.
How Medicare Advantage plans are paid
Medicare Advantage (aka Part-C) is a federal program, where CMS will pay a Medicare Advantage Organization (MAO) a capitated amount of money per-member-per-month (PMPM) to assume the risk of managing that person's healthcare costs. This sounds like, but is not at all like, those calls you get about your car's extended warranty.
Three features of the Medicare Advantage program that deserve your attention are:
- Risk adjustment
- Star ratings
- Quality Bonus Payments (QPBs)
Each of these three create an opportunity for the MAO to receive payments from CMS that are above the "base rate".
Risk adjustment: if plan members are less healthy/more costly than the average member, the MAO will be paid more. So health plans want to make sure that their members are diagnosed with everything they could possibly be diagnosed with. For example, CMS will pay about 4x as much to the MAO for managing the same person after they've been diagnosed with rheumatoid arthritis[1]
Star ratings: CMS grades plans across a range of 46 quality measures, and distills them down into a 5-star scale (in 1/2 star increments). These include things like: Did members get a breast cancer screening? Do diabetic members have their blood sugar under control? Is the customer service good? In 2021, 77% of Medicare Advantage enrollees were in a plan that had 4-stars or more (leaving 23% in plans with 3.5-stars or less)[2].
Quality bonus payment (QBP): Plans that achieve 4 or more stars receive a bonus payment (up to 5% of the benchmark)[3]. The bonus payment doesn't go to the MOA's bottom line, it must be used to reduce member cost sharing, or to pay for "supplemental benefits". Using the industry rule of thumb, $1,000 is a good approximation of the benchmark. So by achieving 4-stars, the MAO can expect an additional $50 PMPM to improve their plan. With 24.1 million people enrolled in Medicare Advantage plans[4], and 23% of them in plans that didn't achieve 4-stars, collectively these plans are leaving ~$3.3BN per year on the table (24.1MM * 23% * $50 * 12).
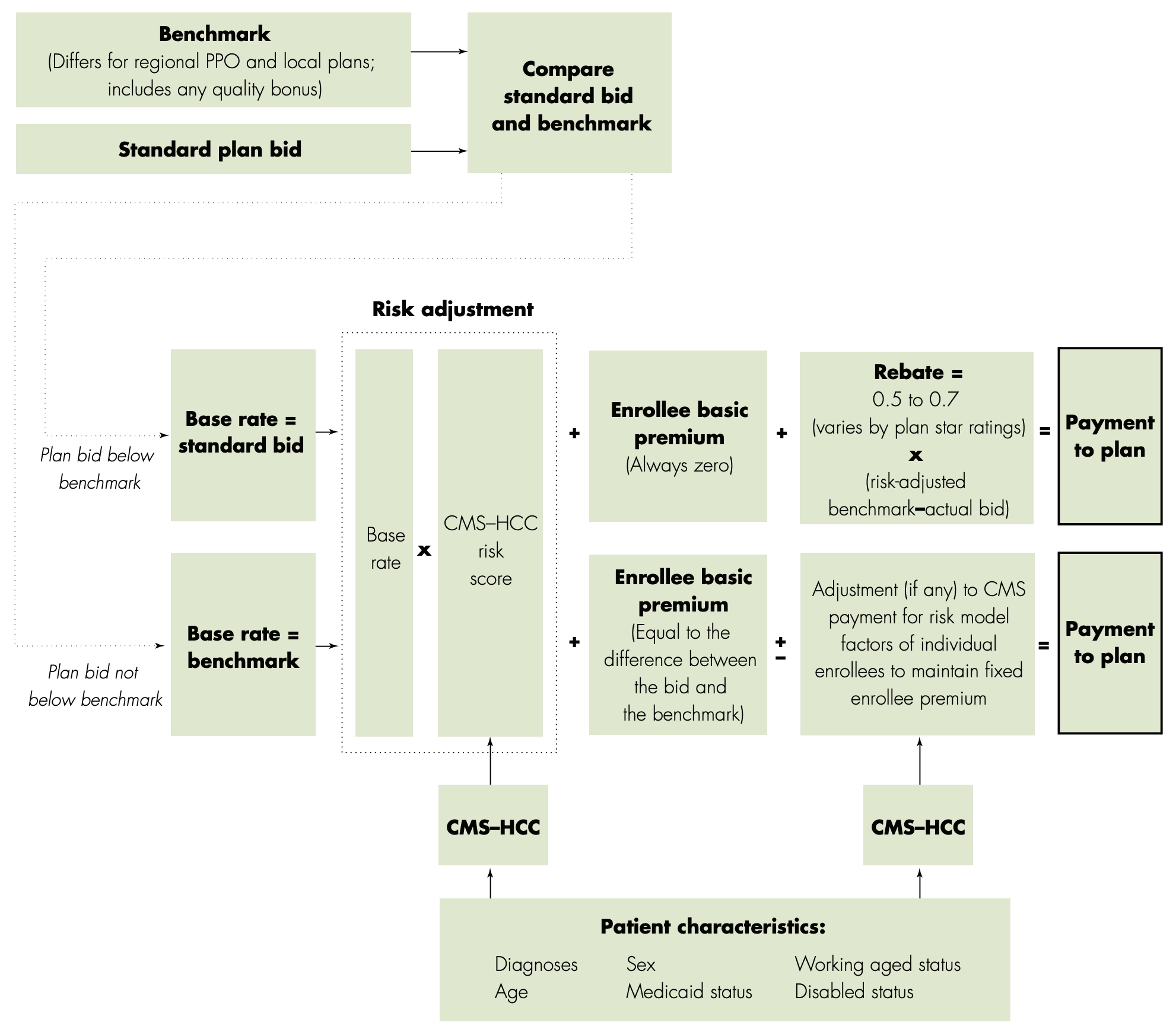
How Medicare Advantage plans are paid. Risk adjustment, Star Ratings, and QBP are opportunities to get paid more than the bid amount [image credit]
If I ran a health plan
"It’s a pretty good zoo," Said young Gerald McGrew, "And the fellow who runs it Seems proud of it too. But if I ran the zoo," Said young Gerald McGrew, "I’d make a few changes. That’s just what I’d do.
Some things I might do if I ran an Medicare Advantage plan:
- I'd create a mandatory supplement benefit that pays the member when they get their free annual wellness visit. This is probably a visa gift card that can be used to pay for any other covered services. My health plan pays YOU when you go to the doctor. As a bonus, the weighting of the "patient experience" category for star ratings is going up from 2 to 4[5], and who wouldn't love an insurance plan that pays you money?
- To take advantage of the risk scoring. I'd create a health plan that is really cost effective at treating rheumatoid arthritis or other highly risk-scored conditions. Then I'd go recruit patients with the condition, in a reverse selection bias. I'd then leverage all my members against the TNF blocker drug class (Humira is about to become the best selling drug in the history of the world) and drive my drug prices down.
- I'd use the patient access and interoperability APIs (which are outside of HIPAA) to connect my plan's patients who have similar medical histories with each other. The plan members also have a vested interest in keeping their costs low. I'd encourage them to share tips with each other.
I'm sure some of these are already being done by MAOs. Maybe some of these are against the rules. But this my zoo / health plan.
Proof of concept
Let's use some of what we learned about Blue Button 2.0 in the last post to try out a proof of concept. Use the "Click to Try" button below along with the test user credentials.
Your personal test user (reload the page for a new one):
| User Name | Password |
|---|---|
|
|
Note: the data in Blue Button 2.0 is for original fee-for-service Medicare and MA-PDP, so it wouldn't actually be applicable for risk adjustment, star ratings, or QBP.
What it did
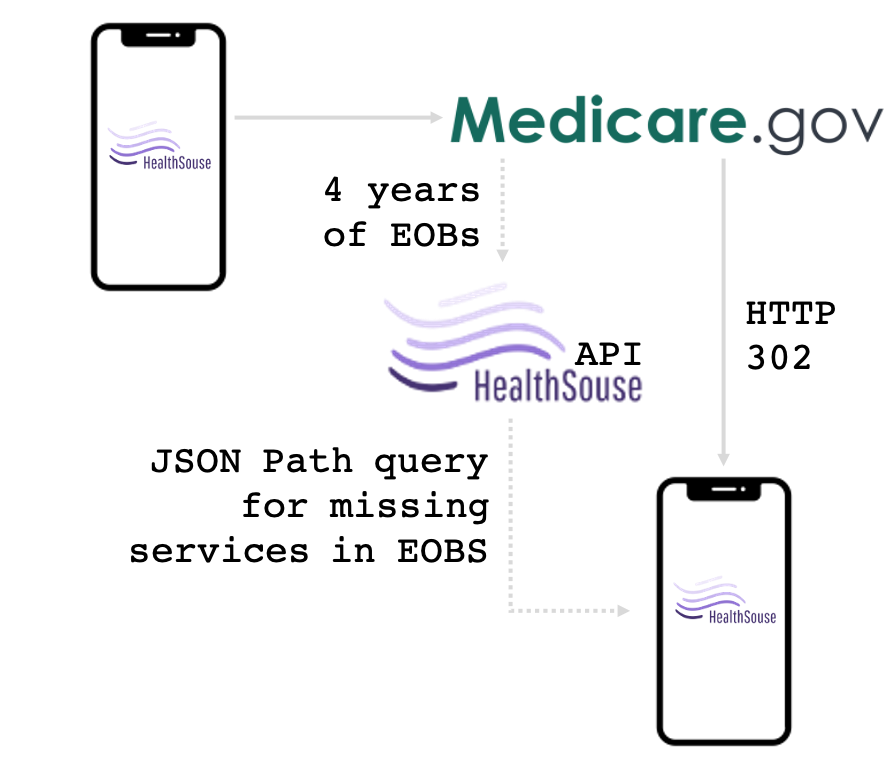
This proof of concept:
- Had you authorize through medicare.gov
- Pulled down the EOB record for your test patient
-
Analyzed the EOB to look for:
- Missing services that would have been available at $0 cost to the patient
- Could have created an opportunity for the plan to improve it's star ratings
- Could have been an opportunity for a new diagnosis that would increase the risk score for this patient.
Wrapping up
And boy! When I get him back home to my park, The whole world will say, 'Young McGrew’s made his mark.'
If I ran a health plan, I'd take a contrarian thesis and try to invert all of the usual expectations you have of an insurance company:
- Can we pay people when they go to the doctor, rather than charge them?
- Can we select for the sickest people, rather than the most healthy?
- Can we use patient access APIs to tie all of them together into a support network that drives higher profits for our health plan, and better health for our members?
A boy can dream.
Do you know someone with an Aetna Medicare Advantage plan? Please send them to the HealthSouse home page. We may also be able to save your friend some money.
Still here? Thanks for reading! You seem like a nice person, who should send me an email: mark@healthsouse.com. Encouragement and criticism are both welcome!
Popular Posts


Humana's patient access APIs
1 August, 2021
Using Blue Button 2.0 - If I ran a health plan
11 June, 2021
Cigna - patient access APIs
18 April, 2021
United / Optum - patient access APIs
18 April, 2021
Oscar, Clover, and Alignment - patient access APIs
04 April, 2021
Patient access scorecard by insurance company
14 March, 2021
